TSH suppression is common among the patients who are treated with NDT (Natural Desiccated Thyroid). TSH stands for Thyroid Stimulating Hormone and is produced by the pituitary gland in the brain. The simplistic view of produced hormones looks like this:
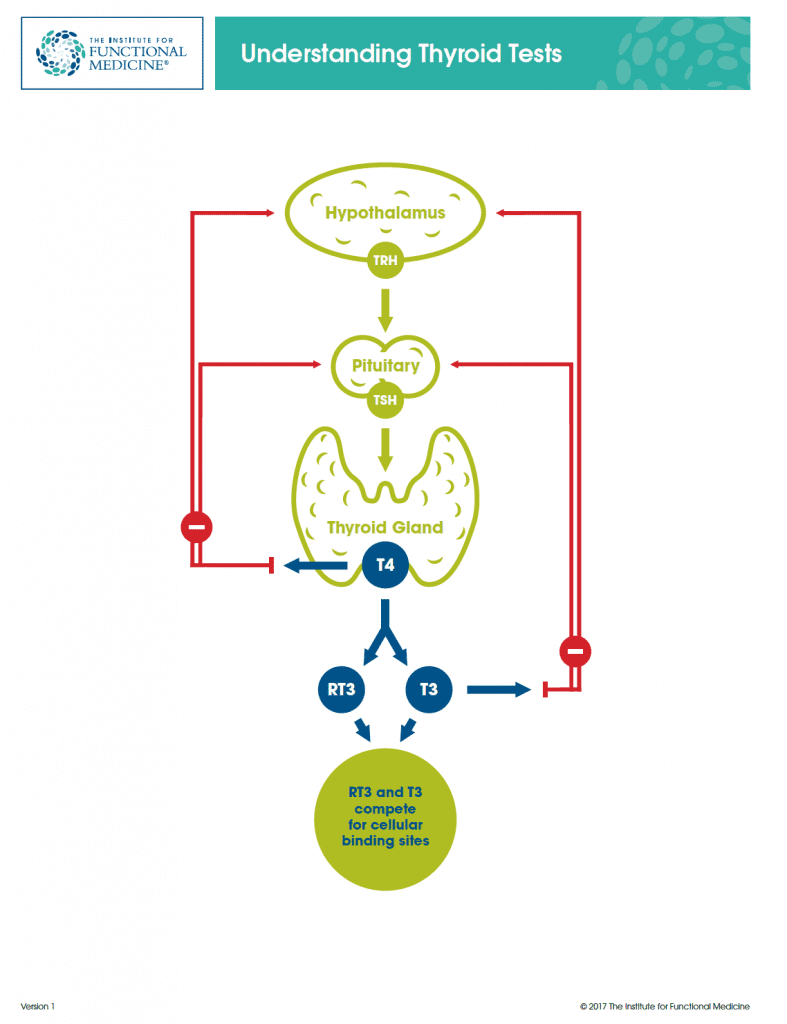
TSH is not a thyroid hormone per se; TSH stimulates the thyroid gland to produce thyroid hormone. Thus, judging the level of the active thyroid hormone (Free T3) by the level of Thyroid STIMULATING Hormone (TSH) just does not make sense.
Unfortunately, the laboratory analysis of blood is just a part of the picture. The most important point is that the person should see the improvement in the hypothyroid symptoms and no side effects with the increase in thyroid hormone dose. The common side effects to watch out for are the heart palpitations, increased anxiety, fast heart rate, jitteriness, and increased irritability. Basically, it just feels like you had way too much coffee. The good thing about dosing NDT is that as soon as the dose is decreased the side effects go away. The symptoms of overdose do not last 6 weeks as it may happen with adjusting T4-only (levothyroxine) medication. The overdosing symptoms are mostly due to the effects of T3 hormone which reaches the body around 2 hours and lasts for about 5 hours after the NDT hormone was taken.
The most common NDT (Natural Desiccated Thyroid) hormone formulations available in the U.S. are NP Thyroid, Armour Thyroid, Nature-Thyroid, and WP Thyroid. Nature-Thyroid is slowly making its’ comeback from a long-standing backorder. Hooray!
So, what happens when you have had a sufficient amount of Free T3 hormone floating in your body? The negative feedback loop to your thyroid gets suppressed, i.e. TSH gets suppressed in most cases.
High TSH – Low Free T3
Low TSH – Sufficient Free T3
Admittedly, there are a number of cases where TSH is within normal or even on the lower end (0.45 – 1.0) while Free T3 is low too. In such cases, exploring the HPA-Axis and its’ malfunction may help to pin down the cause of low thyroid hormone production and why the pituitary is not hurrying up with the production of the TSH to increase the production of thyroid hormone by the thyroid gland. (Sorry, there are a lot of “thyroid” words here, but I am just trying to make it more comprehensible and less confusing).
How safe is it to suppress TSH? Why do healthcare professionals treat to the “optimal” TSH range of 1.0 – 2.0 (or even higher) while not paying the attention to the level of Free T4 and Free T3 hormone and the symptoms that you experience?
Let’s review some available research!
- “Suppressed TSH levels secondary to thyroxine replacement therapy are not associated with osteoporosis” In this study, patients treated with thyroxine (generic levothyroxine) experienced a clinically insignificant reduction in bone mineral density. This small decrease in bone density “should not on its own be an indication for reduction of thyroxine dose in patients who are clinically euthyroid.”
- “Case report: fast reversal of severe osteoporosis after correction of excessive levothyroxine treatment and long-term follow-up” Here is one case study where the patient developed stress fractures due to overdosing on levothyroxine (300 mcg), TSH < 0.0001. Unfortunately, this study did not measure Free T3 – the level of an active hormone that actually is used by the body. The case study only measured TSH, Free T4, and Total T3. As evidenced by this study, Free T4 was out of the normal lab range for this patient when she presented with the bone fractures. “Serum free T4 and TSH should be kept within the reference range for the usual regimen of levothyroxine replacement in hypothyroidism.” Nevertheless, if the patient was diagnosed with thyroid cancer, the research states that the dosage of levothyroxine used should be high enough to suppress TSH. See: “For patients with thyroid cancer, reference guidelines regarding TSH suppression take into account the severity of the malignancy as well as treatment response. Patients with low-grade malignancy and a structural and biochemical complete response to treatment should be substituted to a TSH level of 0.5 to 2.0 mU/L; patients with incomplete biochemical response or increased risk of relapse to a TSH level of 0.1 to 0.5 mU/L and patients with a high risk of relapse to a TSH level below 0.1 mU/L.”
- The study of “Bone mineral density in premenopausal women receiving levothyroxine suppressive therapy” found that levothyroxine suppressive therapy (TSH suppression), when administered to HYPERthyroid patients with non-toxic goiter, had no significant effect on bone mass.
It is worth mentioning that the patients diagnosed with HYPERthyroidism (high levels of thyroid hormones and very low, suppressed TSH), experience side effects caused by high levels of thyroid hormones: insomnia, heart palpitations, decreased bone density (osteopenia, osteoporosis), fast heart rate, etc.
- The 6-year study of “A Longitudinal Evaluation of the Effects of Thyroxine Therapy on Bone Mineral Density” was performed in the patients who underwent a TOTAL thyroidectomy (removal of the thyroid gland) and were given the dose of levothyroxine that suppressed TSH to the undetectable level. These patients did not develop any ongoing deleterious effect on bone density in lumbar and femoral areas of the skeleton.
- “T3 affects expression of collagen I and collagen cross-linking in bone cell cultures” In order to have healthy strong bones, the optimal levels of thyroid hormones are needed. This study showed that T3 up-regulated genes involved in bone matrix formation and promotes collagen maturation. While low levels of T3 will decrease bone matrix formation, high (supraphysiological levels) of T3 will upregulate the genes responsible for the bone resorption (i.e. destruction) process.
- “Possible Limited Bone Loss with Suppressive Thyroxine Therapy Is Unlikely to Have Clinical Relevance” concluded that “the suppressive T4 therapy does not affect bone mass in patients with nontoxic goiter. In patients with thyroid cancer, limited bone loss was detected. No osteoporotic fractures were documented in any of the patients. The minimal amount of bone loss, which was barely significant, is unlikely to have clinical relevance”.
- Desiccated thyroid taken at the dose of 2 grains or higher would most likely suppress TSH due to the higher level of Free T3 in it. Doses of 3 and 4 grains suppressed TSH and also decreased a combined cortical thickness (CCT) according to the research “Thyroid Supplements: Effect on Bone Mass.” Patients who took 2 grains had a more desirable higher CCT score, in comparison to those who took 3 and 4 grains. There is no information on the levels of Free T3 or even Free T4 in this research,
- “Early postmenopausal bone loss in hyperthyroidism” Untreated hyperthyroidism (caused by increased levels of Free T3 and NOT by low levels of TSH) may cause the increased bone loss in postmenopausal women. As the levels of estrogen fall, its’ bone protective actions decline too.
Only in some cases, low TSH may mean HYPERthyroidism. Unfortunately, in a number of cases, low TSH with normal or LOW Free T3 and Free T4 may indicate pituitary or adrenal issue, not a thyroid issue. This leads to the underdosing of the supplemental thyroid hormone and the persistence of numerous hypothyroid symptoms that interfere with the quality of life of each and every patient. Healthcare providers are reluctant to increase the dose of exogenous (outside of the body) thyroid hormone until the patient’s TSH is suppressed and the patient has no HYPOthyroid symptoms anymore.
As time passes, the patients find themselves getting sicker and sicker, gaining more weight, developing fibromyalgia or chronic fatigue syndrome, experiencing heavy irregular menses, loss of libido, brittle bones, diabetes, depression, etc.
As a rule, not only TSH has to be checked, but also Free T3 and Free T4 and the symptoms should be evaluated. Making sure that Free T3 and Free T4 levels are within normal limits is more important than the level of TSH, in my opinion.